Professor Frank Shann is a highly-qualified and highly-respected medical doctor and researcher based in Melbourne. Read his bio, published for an international intensive care conference he spoke at in October 2019:
Frank Shann, AM, MB, BS, DMedSc, FRACP, FCICM, is an Honorary Staff Specialist in Intensive Care at the Royal Children’s Hospital and a Professorial Fellow in the Department of Paediatrics at the University of Melbourne. Frank worked in Papua New Guinea and Kenya for eight years, and helped set up the WHO Acute Respiratory Infections (ARI) programme which is based on his research in Papua New Guinea. He was director of intensive care at the Royal Children’s Hospital in Melbourne for 20 years. He now studies the off-target effects of vaccines in children in low-income countries. He has published 250 articles, six books and 17 book chapters. Frank is a Member of the Order of Australia and a member of the International Advisory Board of The Lancet.
Professor Shann joins many other esteemed medical researchers internationally who study the non-specific effects of vaccines, such as Dr Peter Aaby (Statens Serum Institut, Denmark)) and Professor Christine Stabell Benn (Professor of Global Health, University of Southern Denmark).
These researchers have found that in areas with high infant mortality, giving live vaccines such as measles vaccine (MV), oral polio vaccine (OPV), TB vaccine (BCG) and smallpox vaccine to babies at an early age saves more infants from death than can be explained by saving them from the target diseases. For example, the OPV has reduced infant mortality in an area where polio does not circulate.
However they have also found that giving non-live vaccines in high-mortality regions, especially the “triple antigen” DTP vaccine for diphtheria, tetanus and pertussis (whooping cough), has increased infant deaths, mainly from pneumonia, sepsis and diarrhoea. A study by Aaby, Stabell Benn and others found infants vaccinated with DTP were 10 times more likely to die from any cause than completely unvaccinated infants, and 5 times more likely to die from any cause if OPV was given at the same time as DTP. See:
The Introduction of Diphtheria-Tetanus-Pertussis and Oral Polio Vaccine Among Young Infants in an Urban African Community: A Natural Experiment (2017)
The authors concluded:
It should be of concern that the effect of routine vaccinations on all-cause mortality was not tested in randomized trials. All currently available evidence suggests that DTP vaccine may kill more children from other causes than it saves from diphtheria, tetanus or pertussis. Though a vaccine protects children against the target disease it may simultaneously increase susceptibility to unrelated infections.
Professor Shann and his work on the non-specific effects of vaccines are introduced in the following TEDx talk given by Professor Stabell Benn—video published in January 2019—about the group’s findings, starting at 11:52 minutes.
Here is the slide with Professor Shann’s recommendations on changing the order vaccines are given in high-mortality regions.
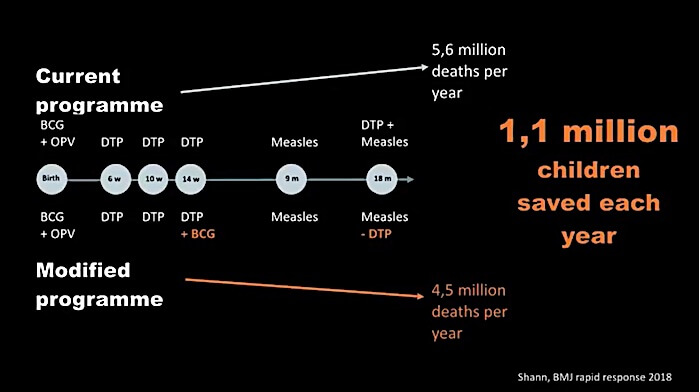 You can see he suggests adding a BCG (a live vaccine) at 14 weeks and removing a DTP (a non-live vaccine) at 18 months. He wouldn’t suggest this if he didn’t believe something was wrong with finishing the sequence with DTP vaccine.
You can see he suggests adding a BCG (a live vaccine) at 14 weeks and removing a DTP (a non-live vaccine) at 18 months. He wouldn’t suggest this if he didn’t believe something was wrong with finishing the sequence with DTP vaccine.
Stabell Benn goes on to say we can save 1.1 million children every year by acting on Shann’s plan, and that’s equivalent to saving more than 3,000 children every day, with minor modification of the vaccination program.
She lists the following non-live vaccines in her video, and says the same non-specific effects have been found for all of them:
- DTP vaccine, for diphtheria, tetanus and pertussis (whooping cough). This vaccine is routinely given in the third world today, but has been replaced in high-income nations including Australia with the DTaP, which is also a non-live vaccine.
- Flu vaccine
- HPV vaccine
- Hepatitis B vaccine
High-income countries
While we would not agree with all of the group’s perspectives, it’s certainly interesting to see what they say. Towards the end of the video (at 12:25 minutes) Stabell Benn says the following:
You may wonder if this has implications in our part of the world, in high-income countries, and it does.
Fortunately, the risk of dying from infections is low here, but many get hospitalised. And when we and others recently started to look for non-specific effects of vaccines on hospitalisations we found exactly the same patterns. For instance in a recent study from the US, children who had a live vaccine had only half the risk of getting hospitalised compared with children who had a non-live vaccine.
So it appears that also in high-income countries we can train our immune systems, we can make ourselves stronger against all kinds of diseases with live vaccines. And this may have implications also for other types of diseases, more chronic diseases, which depend on the immune system, such as asthma and allergies, autoimmune diseases, diabetes, cardiac diseases even some cancers.
So what I’m telling you here is with this new knowledge we can save millions of children in low-income countries and we can reduce disease burden significantly in high-income countries.
It is interesting she is linking chronic conditions such as autoimmune disease, and cancer, with the vaccine issue.
She also says:
We are having a really hard time getting the world to listen.
Nobody ever proved that vaccines only have protective effects. And we’ve been accumulating data for 25 years now showing that vaccines have important non-specific effects. Yet the world only focuses on the protective effects.
She then goes on to speculate why health authorities will not listen to and act on the research findings, suggesting they are not interested because the results “imply the possibility that some vaccines may be harmful.”
Stabell Benn also had an article published in January 2019:
Vaccines have health effects beyond protecting against target diseases
She says:
We have now investigated four live vaccines and six non-live vaccines, in Guinea-Bissau and other low-income countries, as well as in Denmark. A consistent pattern has emerged. The live vaccines reduce death and disease much more than can be explained by the specific protection. But the non-live vaccines, in spite of protecting against the vaccine disease, are associated with negative effects on health, including death, particularly for girls.
Professor Shann’s work
Professor Shann has published widely. He is very pro-vaccine and is an enthusiastic supporter of the use of vaccines, live and non-live, in high-mortality regions.
However he expresses a great deal of concern about the non-specific effects of non-live vaccines; read what he has said about them in the publications listed below. To access whole papers use this website: https://sci-hub.se
The heterologous (non-specific) effects of vaccines: implications for policy in high-mortality countries (2015)
Also find here:
https://sci-hub.se/10.1093/trstmh/tru161
There is very worrying evidence from observational studies that DTP or Penta (DTP, Haemophilus influenzae type b and hepatitis B vaccines) may increase all-cause mortality in girls in high-mortality countries. No studies were performed on the effects of DTP on all-cause mortality before it was recommended for routine use in the EPI programme; we need unequivocal evidence that an intervention is safe before it is administered routinely to entire populations of healthy people. There are numerous examples of interventions that have had a beneficial effect on a specific outcome but increased all-cause mortality; this is particularly important in infants, where many treatments have had disastrous side-effects.
Heterologous vaccine effects (2016)
In this article Professor Frank Shann is a coauthor with Dr Peter Aaby, who is a colleague and life partner of Professor Stabell Benn.
Find the complete article on Sci Hub here:
https://sci-hub.se/10.1016/j.vaccine.2016.06.020
While the specific effects of vaccines are additive and not affected by the sequence of vaccination, the NSEs [non-specific effects] might be determined by the order in which live and non-live vaccines are administrated. For example, several studies in low-income countries including a randomized trial have found that receipt of DTP vaccine rather than MV as the most recent vaccine was associated with increased mortality in girls. In addition, a study in Denmark noted that the incidence rate ratio for infection-related hospital admissions was significantly greater in children who received the third dose of the inactivated DTaP-IPV-Hib vaccine following live MMR vaccine.
BMJ Rapid Response, Re: Non-specific effects of childhood vaccines (2018)
Dr Yung claims that it is beyond debate that diphtheria, tetanus and pertussis (DTP) vaccine is safe, and yet the Higgins Review found that DTP is associated with a 38% (-8% to 108%) increase in mortality – and with a 53% (2% to 130%) increase in mortality if the Papua New Guinea study with extreme survival and/or frailty bias is excluded, as recommended by 2 of the 3 peer reviewers.
Talk at Melbourne’s Royal Children’s Hospital by Frank Shann, “peerless physician”
The State of the World in 2014 – Amazing Progress
Professor Shann speaks about progress in world health over centuries, and significantly he does not mention vaccines once, apart from answering a question at the end by saying he would put money into investigation of the non-specific effects of vaccines.
Live vaccines
At the end of her talk Stabell Benn suggests people who have negative opinions of vaccines are not looking at the positive possibilities suggested by the research. We would say that she and the other researchers seem to be oblivious to the following issues with live vaccines, see references at end of article:
- Immunity obtained from live childhood vaccines wears off, leaving recipients exposed to diseases such as measles, mumps, rubella, and chicken pox when they are adults and much more vulnerable to these illnesses than are young children. Natural immunity to these diseases however lasts a life-time, in most cases.[1] [2] [3]
- For the above diseases, booster immunity lasts for as little as a few months, leaving people vulnerable for a lifetime to diseases that can be very serious in adults.[4]
- Rubella and chicken pox vaccines contain free-floating human foetal DNA, which can be incorporated into stem cells and cause dangerous mutations, including cancer-causing mutations.[5] [6]
- Live vaccines contain retroviruses which plausibly could cause cancer.[7]
- Live vaccines contain contaminants of unknown origin.[8]
- Live vaccines cause inflammation that can precipitate regression into autism.[9] [10] [11] Courts have compensated claimants for autism following the MMR vaccine[12] [13], studies that find the MMR vaccine does not cause autism suffer from healthy user bias because MMR is less likely to be given to children who have reacted badly to earlier vaccines[14] and MMR-autism studies do not include a completely unvaccinated comparison group.[15]
- The studies showing beneficial effects of live vaccines are short term; we need different kinds of studies to investigate problems raised in the above list.
Action
Federal law here in Australia mandates both live and non-live vaccines for low-income family funding, and most states require adherence to the government’s vaccination schedule to enrol pre-school children in childcare and kindergarten. Non-live vaccines feature prominently on the schedule: in the first 6 months of life 23 doses of non-live vaccines are given, at 12 and 18 months live and non-live vaccines are given together, at 4 years a combo shot containing 4 non-live vaccines is given, and year 7 students are assaulted with two non-live vaccines, the Tdap and HPV vaccine Gardasil, as a welcome to their teenage years.
Recently Victoria announced a draconian bill to allow vaccines to be made mandatory for health workers engaged with the public in any way. Three non-live vaccines were mentioned in the Government’s press release: flu, whooping cough, and hepatitis B, (of course, the “whooping cough” vaccine is a vaccine for 3 diseases, the Tdap), but any vaccine deemed at any time to be necessary could be made compulsory for employment under this legislation.
Many parents, doctors and nurses know that non-live vaccines such as the flu vaccine often make people sick from off-target infections, so it’s no surprise many don’t want them – this phenomenon has been known for years, it’s usually called ‘original antigenic sin’ or ‘linked epitope suppression’. (By the way, this means the flu vaccine is likely to make coronavirus COVID-19 infection more serious.)
If this is you, we urge you to show information from this post, perhaps the video or an article, to your MP, a journalist or anyone else you can think of, to make more people aware of the non-specific affects of non-live vaccines. It could at least open people’s eyes to the fact vaccine science isn’t “settled” at all. Read more about the proposed Victorian Health Workers Law and what you can do about it on this page.
We hope Professor Frank Shann speaks to our MPs, especially Victoria’s health minister, about laws mandating vaccines which are known to have negative effects.
Drug Doses
Frank Shann produces a booklet, Drug Doses. It is a reference book apparently used mainly by nurses, and he updates it every few years. He is known for occasionally inserting recipes into the book – find recipes for chocolate cake here and roast potatoes here. It is apparently a “thing” to bake his “cake, diablo” for occasions, and Shann appears to be regarded affectionately by nurses for this quirky contribution to their working life.
References
- Persistence of Measles Antibodies After 2 Doses of Measles Vaccine in a Postelimination Environment
- Early Measles Vaccination During an Outbreak in the Netherlands: Short-Term and Long-Term Decreases in Antibody Responses Among Children Vaccinated Before 12 Months of Age
- Waning Immunity Is Associated with Periodic Large Outbreaks of Mumps: A Mathematical Modeling Study of Scottish Data
- Measles Virus Neutralizing Antibody Response, Cell-Mediated Immunity, and Immunoglobulin G Antibody Avidity Before and After Receipt of a Third Dose of Measles, Mumps, and Rubella Vaccine in Young Adults
- DNA FRAGMENTS RESEARCH
- MMRV Contains 100 Chemical Contaminants and DNA of Male Human Being
- Investigating Viruses in Cells Used to Make Vaccines; and Evaluating the Potential Threat Posed by Transmission of Viruses to Humans
- Corvelva – Summary of data confirmations through interlaboratory analysis
- Measles Inclusion-Body Encephalitis Caused by the Vaccine Strain of Measles Virus
- Antibody-Mediated Encephalitis
- The Spectrum of Post-Vaccination Inflammatory CNS Demyelinating Syndromes
- Family to Receive $1.5M+ in First-Ever Vaccine-Autism Court Award
- MMR: A mother’s victory. The vast majority of doctors say there is no link between the triple jab and autism, but could an Italian court case reignite this controversial debate?
- Healthy User Bias: The Fatal Flaw in Vaccine Safety Research
- Meta-Analysis Madness in Vaccine-Autism Science

Leave a Reply